Vision is not merely a sensory function, it is the architecture through which we interpret detail, depth, and meaning. When central vision begins to erode, the impact is not sudden chaos but a gradual distortion, like a painting losing its sharpest lines. This is the clinical reality of macular degeneration, a progressive retinal disorder that selectively compromises the macula, the region responsible for high-acuity vision.
Among its classifications, age-related macular degeneration (AMD) manifests in two primary forms: dry (non-neovascular) and wet (neovascular). While both share a common endpoint, central vision loss, their underlying mechanisms, clinical progression, and management strategies differ significantly.
Understanding the Pathophysiology
Dry AMD (Non-Neovascular)
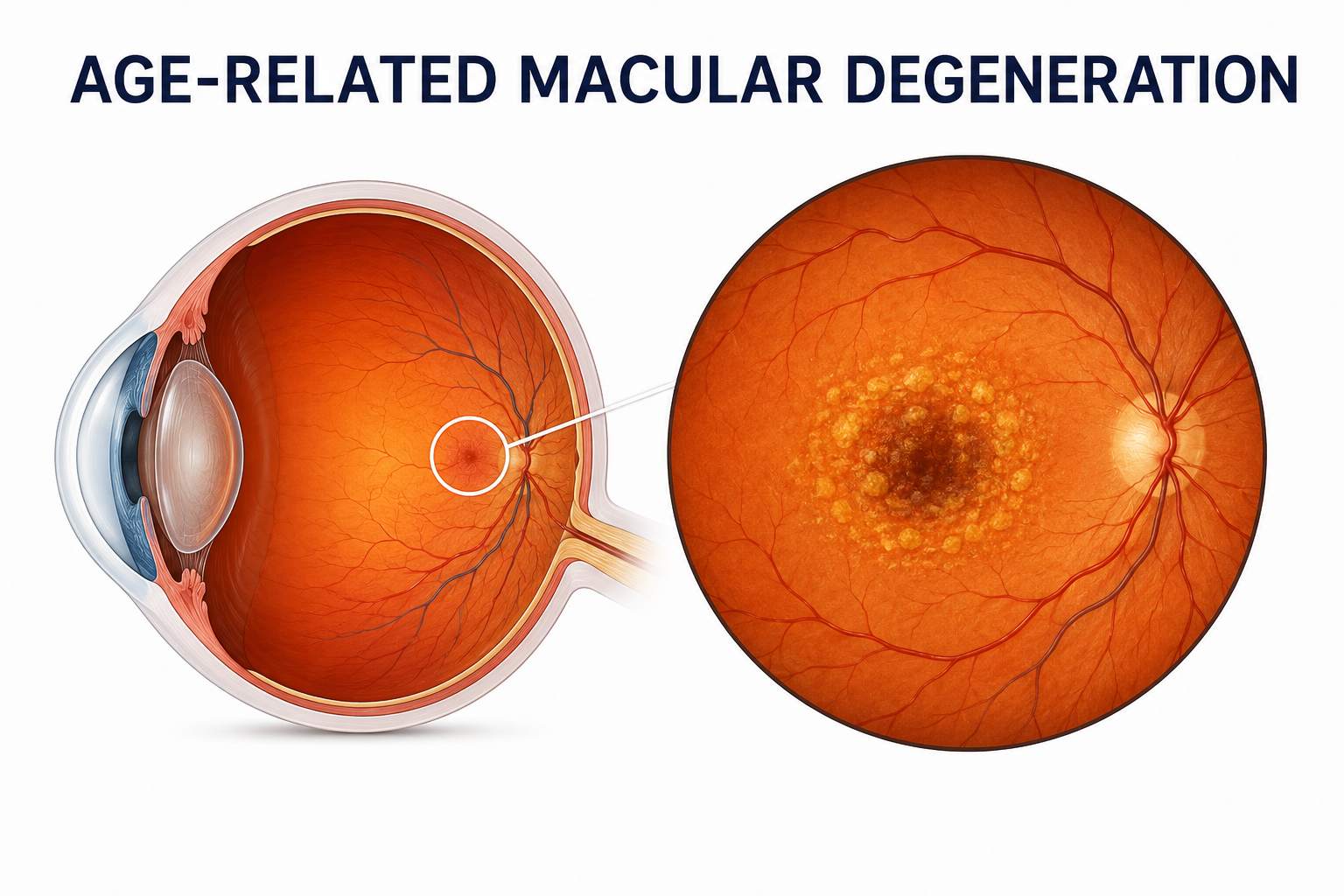
Dry AMD accounts for approximately 80–90% of all cases of age-related macular degeneration. Its pathogenesis is insidious and multifactorial. The hallmark feature is the accumulation of extracellular deposits known as drusen between the retinal pigment epithelium (RPE) and Bruch’s membrane.
Over time, these deposits disrupt metabolic exchange, leading to:
- Progressive RPE dysfunction.
- Photoreceptor degeneration.
- Thinning (atrophy) of the macula.
In advanced stages, this culminates in geographic atrophy, a well-demarcated loss of retinal tissue that directly impairs central vision.
Wet AMD (Neovascular)
Wet AMD is less common but significantly more aggressive. It arises from pathological angiogenesis triggered by vascular endothelial growth factor (VEGF). In this form of macular degeneration, abnormal blood vessels proliferate beneath the retina.
These vessels are structurally fragile and prone to:
- Leakage of fluid.
- Hemorrhage.
- Fibrotic scarring.
The result is rapid and often irreversible damage to the macula, leading to acute visual distortion and central vision loss.
Clinical Presentation and Symptoms
Symptoms of Dry AMD
Dry AMD progresses gradually, often delaying detection in its early stages. Patients may report:
- Blurred or hazy central vision.
- Difficulty recognizing faces.
- Increased need for bright lighting.
- Reduced contrast sensitivity.
As the disease advances, central blind spots (scotomas) may develop, particularly in cases progressing to geographic atrophy.
Symptoms of Wet AMD
Wet AMD presents more abruptly and is clinically more alarming. Key symptoms include:
- Sudden distortion of straight lines (metamorphopsia).
- Rapid decline in central vision.
- Dark or empty areas in the visual field.
- Reduced color perception.
An Amsler grid test often reveals wavy or missing lines, serving as an early indicator of neovascular activity.
Diagnostic Approach
Timely differentiation between dry and wet forms of age-related macular degeneration is critical for prognosis and treatment planning. Standard diagnostic modalities include:
- Optical Coherence Tomography (OCT): Provides cross-sectional imaging of retinal layers, identifying drusen, fluid accumulation, and structural damage.
- Fundus Fluorescein Angiography (FFA): Essential for detecting choroidal neovascularization in wet AMD.
- Fundus Examination: Reveals drusen in dry AMD and hemorrhages or exudates in wet AMD.
Treatment Protocols
Management of Dry AMD
Currently, there is no definitive cure for dry macular degeneration, but progression can be slowed through targeted interventions:
- Nutritional Supplementation
The AREDS 2 (Age-Related Eye Disease Study) formulation is the gold standard for intermediate to advanced dry AMD. It includes:
- Vitamin C and E
- Zinc
- Copper
- Lutein and zeaxanthin
These antioxidants mitigate oxidative stress, a key contributor to retinal degeneration.
- Lifestyle Modifications
Patients are advised to:
- Cease smoking (a major risk factor).
- Maintain a diet rich in leafy greens and omega-3 fatty acids.
- Manage systemic conditions such as hypertension.
- Emerging Therapies
Recent advances include complement pathway inhibitors targeting inflammatory mechanisms involved in geographic atrophy. These therapies are reshaping the future landscape of dry AMD management.
Management of Wet AMD
Wet AMD requires urgent and aggressive treatment to preserve vision. The cornerstone of therapy is anti-VEGF pharmacotherapy.
- Intravitreal Anti-VEGF Injections
Agents such as ranibizumab, aflibercept, and bevacizumab inhibit VEGF, thereby:
- Preventing new vessel formation.
- Reducing vascular permeability.
- Stabilizing or improving vision.
Treatment is typically administered monthly or via treat-and-extend protocols based on disease activity.
- Photodynamic Therapy (PDT)
Though less commonly used today, PDT involves the activation of a photosensitizing agent (verteporfin) with laser light to selectively destroy abnormal vessels.
- Laser Photocoagulation
Reserved for specific cases, this method seals leaking vessels but carries a risk of collateral retinal damage.
Prognosis and Disease Monitoring
The prognosis of age-related macular degeneration depends largely on early detection and adherence to treatment. Dry AMD progresses slowly but can lead to significant vision impairment over time. Wet AMD, while aggressive, can often be controlled effectively with timely anti-VEGF therapy.
Regular follow-up, including OCT imaging and self-monitoring with Amsler grids, is essential for both forms.
Final Perspective
The distinction between dry and wet macular degeneration is not merely academic, it dictates the clinical trajectory and therapeutic urgency. While dry AMD reflects a chronic degenerative process, wet AMD represents an acute vascular pathology requiring immediate intervention.
As research advances, the boundary between management and restoration continues to shift. For now, the most effective strategy remains a combination of early diagnosis, patient education, and evidence-based treatment protocols, preserving not just vision, but the clarity with which life is experienced.





